
FRAX Adjusted for TBS
By Dr Andrew J. Laster, Rheumatologist AOCC Arthritis & Osteoporosis Consultants of the Carolinas Charlotte, North Carolina 28 207, USA

Patient Clinical Background
This is a 57-year old postmenopausal white female with a 12-year history of rheumatoid arthritis currently in remission on q eight-month IV rituximab, prednisone 5 mg QAM and diclofenac 75 mg daily. She was recently seen after sustaining bilateral low trauma forearm fractures when she tripped in church.
Her BMI is 23.9. She denies a history of prior fractures as an adult. She neither smokes nor drinks and has no other known risk factors for osteoporosis aside from nulliparity, rheumatoid arthritis and low-dose prednisone use. On exam she was noted to have lost 2″ in height compared to known historical baseline. Her laboratory studies were significant only for an elevated CRP of 1.1 mg/deciliter. She had a normal CBC, chemistry profile, TSH, PTH, 25 OH vitamin D, SPEP, 24-hour urine calcium and urine N-telopeptide. No vertebral fractures were seen on VFA.
Bone Assessment & Analysis Images
Osteoporotic BMD
Spine T-Score (L1-L4 ): -3.2
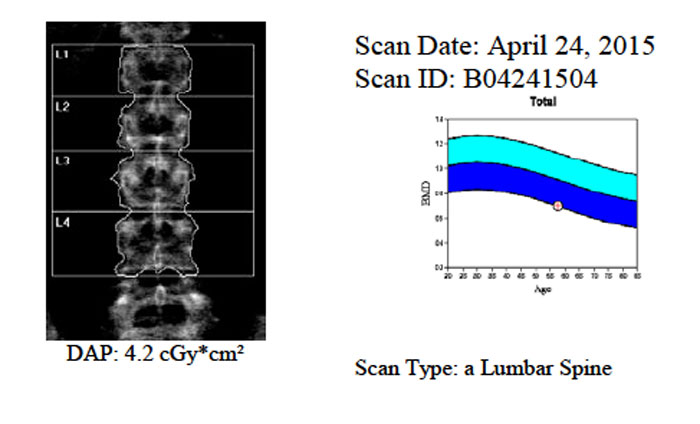
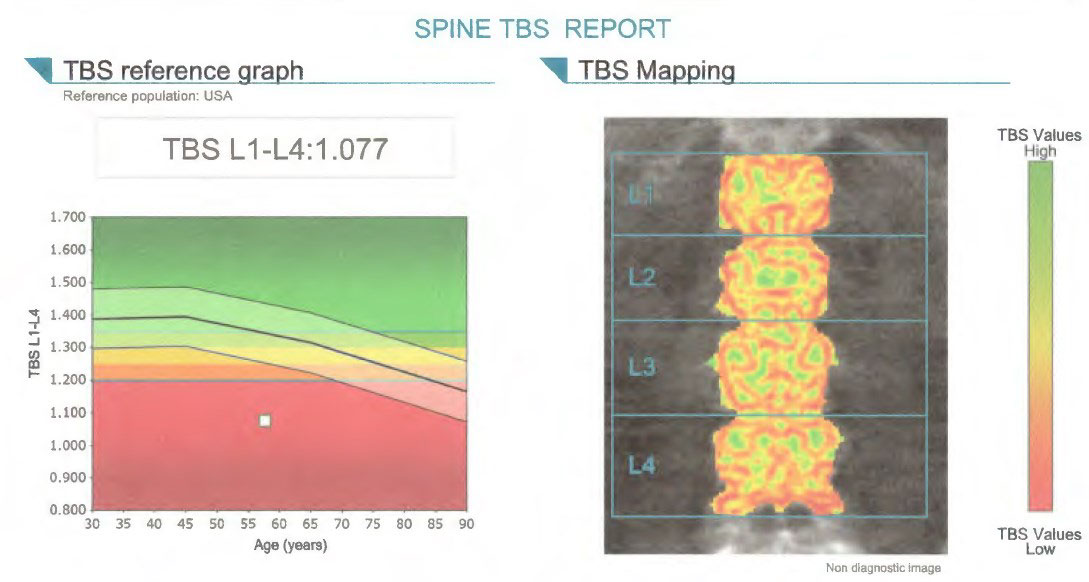
Low TBS Value
Spine TBS (L1-L4): 1.077
FRAX 10-year & FRAX Adjusted for TBS Assessments
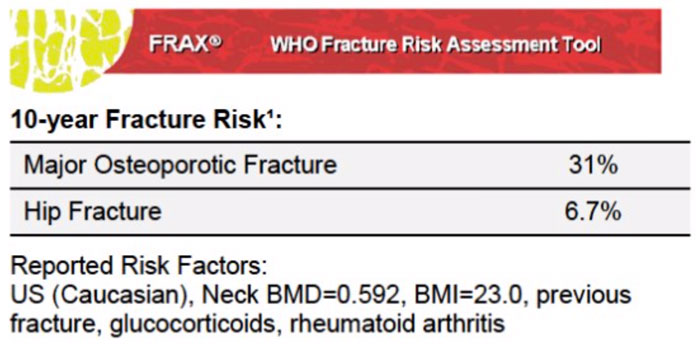
The 10 year probability of fracture (%) Adjusted for TBS
Major Osteoporotic Fracture: 38
Hip Fracture : 12
Conclusion & Patient Management Decision
The patient has osteoporosis based on recent fragility fractures of bilateral forearms. Her baseline DXA study shows densitometric evidence of osteoporosis with a lowest T-score of -3.2 in the lumbar spine. VFA did not identify any vertebral compression fractures. Risk factors include a history of rheumatoid arthritis, nulliparity and low-dose prednisone. No other secondary causes of metabolic bone disease were identified.
The profoundly low TBS results in a near doubling of the 10-year risk of hip fracture when TBS is modeled with FRAX® as compared to modeling with FRAX® alone (see above) in this individual. This finding reinforced the author’s recommendation to initiate therapy with the only anabolic drug currently available in the USA, teriparatide 20 μg daily for two years. Based on the reported clinical and laboratory findings, her insurance company did not require prior treatment with an oral bisphosphonate or other parenteral drug therapies approved for the treatment of osteoporosis.